In vitro fertilization (IVF) involves several steps — ovulation induction, egg retrieval, sperm retrieval, fertilization and embryo transfer. One cycle of IVF can take about two weeks, and more than one cycle may be required.
Ovulation induction
If you're using your own eggs during IVF, at the start of a cycle you'll begin treatment with synthetic hormones to stimulate your ovaries to produce multiple eggs — rather than the single egg that normally develops each month. Multiple eggs are needed because some eggs won't fertilize or develop normally after fertilization.
You may need several different medications, such as:
-
Medications for ovarian stimulation. To stimulate your ovaries, you might receive an injectable medication containing a follicle-stimulating hormone (FSH), a luteinizing hormone (LH) or a combination of both. These medications stimulate more than one egg to develop at a time.
-
Medications for oocyte maturation. When the follicles are ready for egg retrieval — generally after eight to 14 days — you will take human chorionic gonadotropin (HCG) or other medications to help the eggs mature.
-
Medications to prevent premature ovulation. These medications prevent your body from releasing the developing eggs too soon.
-
Medications to prepare the lining of your uterus. On the day of egg retrieval or at the time of embryo transfer, your doctor might recommend that you begin taking progesterone supplements to make the lining of your uterus more receptive to implantation.
Your doctor will work with you to determine which medications to use and when to use them.
Typically, you'll need one to two weeks of ovarian stimulation before your eggs are ready for retrieval. To determine when the eggs are ready for collection, your doctor will likely perform:
-
Vaginal ultrasound, a procedure that uses sound waves to create an image of your ovaries to monitor the development of fluid-filled ovarian sacs where eggs mature (follicles)
-
Blood tests to measure your response to ovarian stimulation medications — estrogen levels typically increase as follicles develop and progesterone levels remain low until after ovulation
Sometimes IVF cycles need to be canceled before egg retrieval for one of these reasons:
-
Inadequate number of follicles developing
-
Premature ovulation
-
Too many follicles developing, creating a risk of ovarian hyperstimulation syndrome
-
Other medical issues
If your cycle is canceled, your doctor might recommend changing medications or their dose to promote a better response during future IVF cycles. Or you may be advised that you need an egg donor.
Egg retrieval
Egg retrieval can be done in your doctor's office or a clinic 34 to 36 hours after the final injection and before ovulation.
-
During egg retrieval, you'll be sedated and given pain medication.
-
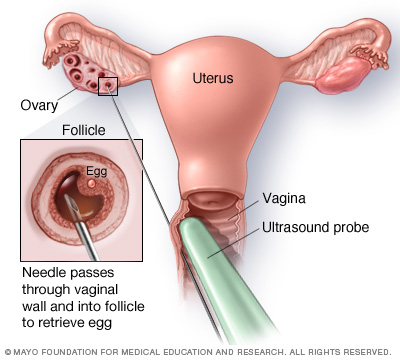
Transvaginal ultrasound aspiration is the usual retrieval method. An ultrasound probe is inserted into your vagina to identify follicles. Then a thin needle is inserted into an ultrasound guide to go through the vagina and into the follicles to retrieve the eggs.
-
If your ovaries aren't accessible through transvaginal ultrasound, an abdominal surgery or laparoscopy — a procedure in which a tiny incision is made near your navel and a slender viewing instrument (laparoscope) is inserted — may be used to guide the needle.
-
The eggs are removed from the follicles through a needle connected to a suction device. Multiple eggs can be removed in about 20 minutes.
-
After egg retrieval, you may experience cramping and feelings of fullness or pressure.
-
Mature eggs are placed in a nutritive liquid (culture medium) and incubated. Eggs that appear healthy and mature will be mixed with sperm to attempt to create embryos. However, not all eggs may be successfully fertilized.
Sperm retrieval
If you're using your partner's sperm, he'll provide a semen sample at your doctor's office or a clinic through masturbation the morning of egg retrieval. Other methods, such as testicular aspiration — the use of a needle or surgical procedure to extract sperm directly from the testicle — are sometimes required. Donor sperm also can be used. Sperm are separated from the semen fluid in the lab.
Fertilization
Fertilization can be attempted using two common methods:
-
Insemination. During insemination, healthy sperm and mature eggs are mixed and incubated overnight.
-
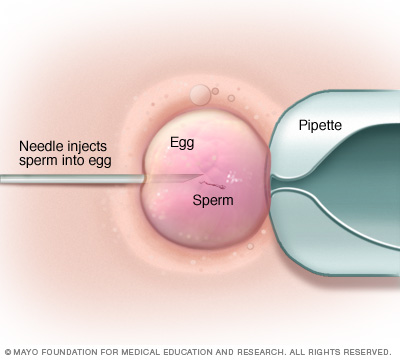
Intracytoplasmic sperm injection (ICSI). In ICSI, a single healthy sperm is injected directly into each mature egg. ICSI is often used when semen quality or number is a problem or if fertilization attempts during prior IVF cycles failed.
In certain situations, your doctor may recommend other procedures before embryo implantation.
-
Assisted hatching. About five to six days after fertilization, an embryo "hatches" from its surrounding membrane (zona pellucida), allowing it to implant into the lining of the uterus. If you're an older woman, or if you've have had multiple failed IVF attempts, your doctor might recommend assisted hatching — a technique in which a hole is made in the zona pellucida just before implantation to help the embryo hatch and implant.
-
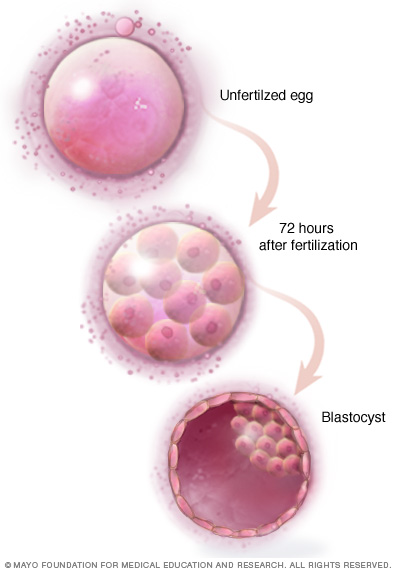
Preimplantation genetic testing. Embryos are allowed to develop in the incubator until they reach a stage where a small sample can be removed and tested for specific genetic diseases or the correct number of chromosomes, typically after five to six days of development. Embryos that don't contain affected genes or chromosomes can be implanted in your uterus. While preimplantation genetic testing can reduce the likelihood that a parent will pass on a genetic problem, it can't eliminate the risk. Prenatal testing may still be recommended.
Embryo transfer
Embryo transfer is done at your doctor's office or a clinic and usually takes place two to six days after egg retrieval.
-
You might be given a mild sedative. The procedure is usually painless, although you might experience mild cramping.
-
The doctor or nurse will insert a long, thin, flexible tube called a catheter into your vagina, through your cervix and into your uterus.
-
A syringe containing one or more embryos suspended in a small amount of fluid is attached to the end of the catheter and then delivered through the tube into your uterus.
If successful, the embryo will implant in the lining of your uterus about six to 10 days after egg retrieval.
After the procedure
After the embryo transfer, you can resume your normal daily activities. However, your ovaries may still be enlarged. Consider avoiding vigorous activity, which could cause discomfort.
Typical side effects include:
-
Passing a small amount of clear or bloody fluid shortly after the procedure — due to the swabbing of the cervix before the embryo transfer
-
Breast tenderness due to high estrogen levels
-
Mild bloating
-
Mild cramping
-
Constipation
If you develop moderate or severe pain after the embryo transfer, contact your doctor. He or she will evaluate you for factors such as infection, twisting of an ovary (ovarian torsion) and severe ovarian hyperstimulation syndrome.